





 |
 |
| J Korean Med Assoc > Volume 52(3); 2009 > Article |
Abstract
Lipid particles, which can be synthesized in the liver or absorbed through the terminal ileum, are indispensable for maintaining homeostasis. Inadequate life styles together with certain types of genetic background can induce and aggravate the condition of dyslipidemia. The personal status of inflammation, which is reflected by the serum C-reactive protein level, and the status of insulin resistance are considered as emerging risks for cardiovascular diseases. Therefore, together with aggressive management of correctable major risks, maintaining ideal lifestyles may be helpful to prevent the event of cardiovascular diseases. The most important goal of managing dyslipidemic conditions is to reach an ideal level of lipid profile, and aggressive drug management can be tried where indicated.
Acknowledgements
This work was supported by the Korea Science and Engineering Foundation (KOSEF) grant funded by the Korean government(MOST) (No. M10748000263-07N4800-26310). KH Han and SH Lim were in part supported by grant A050020 from the Korean Ministry of Health and Welfare, 2009-288 from the Asan Institute for Life Sciences and by the Cardiovascular Research Foundation, Seoul, Korea.
References
1. Thompson GR. A handbook of hyperlipidemia 1990;London: Current Science Ltd.
2. Hovingh GK, de Groot E, van der Steeg W, Boekholdt SM, Hutten BA, Kuivenhoven JA, Kastelein JJ. Inherited disorders of HDL metabolism and atherosclerosis. Curr Opin Lipidol 2005;16:139-145.
3. Brousseau ME, Schaefer EJ, Wolfe ML, Bloedon LT, Digenio AG, Clark RW, Mancuso JP, Rader DJ. Effects of an inhibitor of cholesteryl ester transfer protein on HDL cholesterol. N Engl J Med 2004;350:1505-1515.
4. National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-3421.
15. Danesh J, Wheeler JG, Hirschfield GM, Eda S, Eiriksdottir G, Rumley A, Lowe GD, Pepys MB, Gudnason V. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
6. Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ. JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359(21):2195-2207.
7. Griffin BA, Caslake MJ, Yip B, Tait GW, Packard CJ, Shepherd J. Rapid isolation of low density lipoprotein (LDL) subfractions from plasma by density gradient ultracentrifugation. Atherosclerosis 1990;83:59-67.
8. Cho HK, Jang YS. Small dense LDL and atherosclerotic disease. Korean Journal of Lipid and Atherosclerosis 2003;2:360-315.
9. Piepho RW. The pharmacokinetics and pharmacodynamics of agents proven to raise high-density lipoprotein cholesterol. Am J Cardiol 2000;86:35L-40L.
Figure 3
Risk assessment in primary prevention of cardiovascular disease (CVD); The effects of high-Sensitivity C-reactive protein and the ratio of total cholesterol (TC) and high density lipoprotein cholesterol (HDL-C)
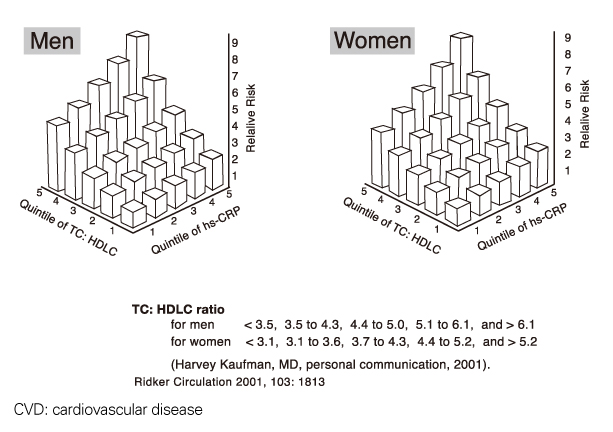
Figure 5
LDL particle size and apolipoprotein B predict ischemic heart disease: Quebec Cardiovascular Study.
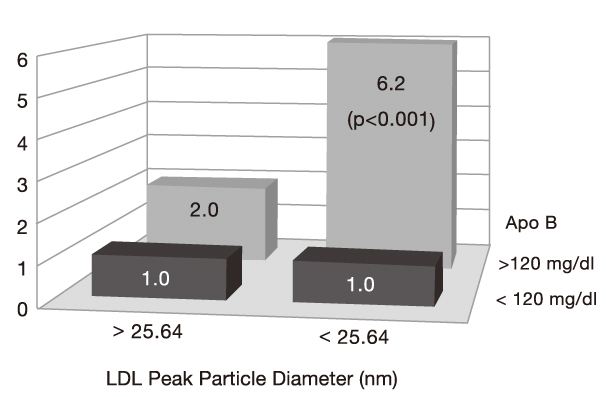
Table 1
Major risk factors for candiovascular disease other than LDL cholestenol level (NCEP-III guideline)
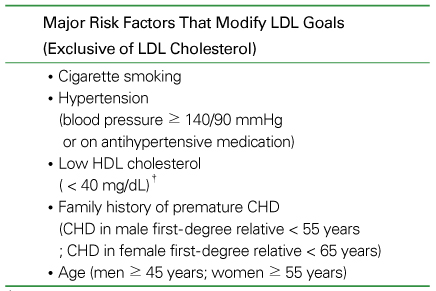
Table 3
Definition of metabolic syndrome (NCEP-III guideline) (≥ 3 factors fulfills the diagnosis)
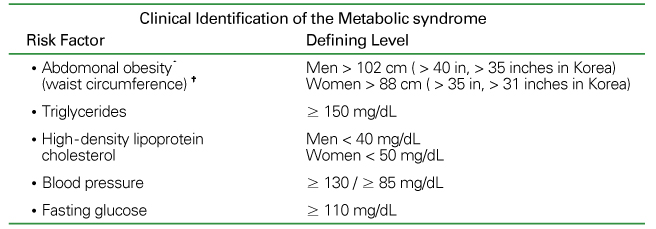
*Overweight and obesity are associated with insulin resistance and the metabolic syndrome. However, the presence of abdominal obesity is more highly correlated with the metabolic risk factors than is an elevated body mass index (BMI). Therefire, the simple measure of waist circumference is recommended to identify the body weight component of the metabolic syndrome.
†Some male patients can develop multiple metabolic risk factors when the waist circumference is only marginally increased, eg, 94~102 cm (37~40 in) Such patients may have strong genetic contribution to insulin resistance and they should benefit from changes in life habits, similarly to men with categorical increases in waist circumference.
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Drug Therapy of Dyslipidemia1998 December;41(12)
Functional Dyspepsia1999 September;42(9)
Drug Therapy of Dyslipidemia2001 July;44(7)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
